A 70-year-old woman presented with left lower back pain and radiation to the left leg on the background of prior surgery to the L3/4 level on the right with rhizolysis.
HISTORY
A 70-year-old woman presented with left lower back pain and radiation to the left leg on the background of prior surgery to the L3/4 level on the right with rhizolysis.
Comparison of the current 2019 MRI was made with the previous MRI from 2011.
IMAGE FINDINGS
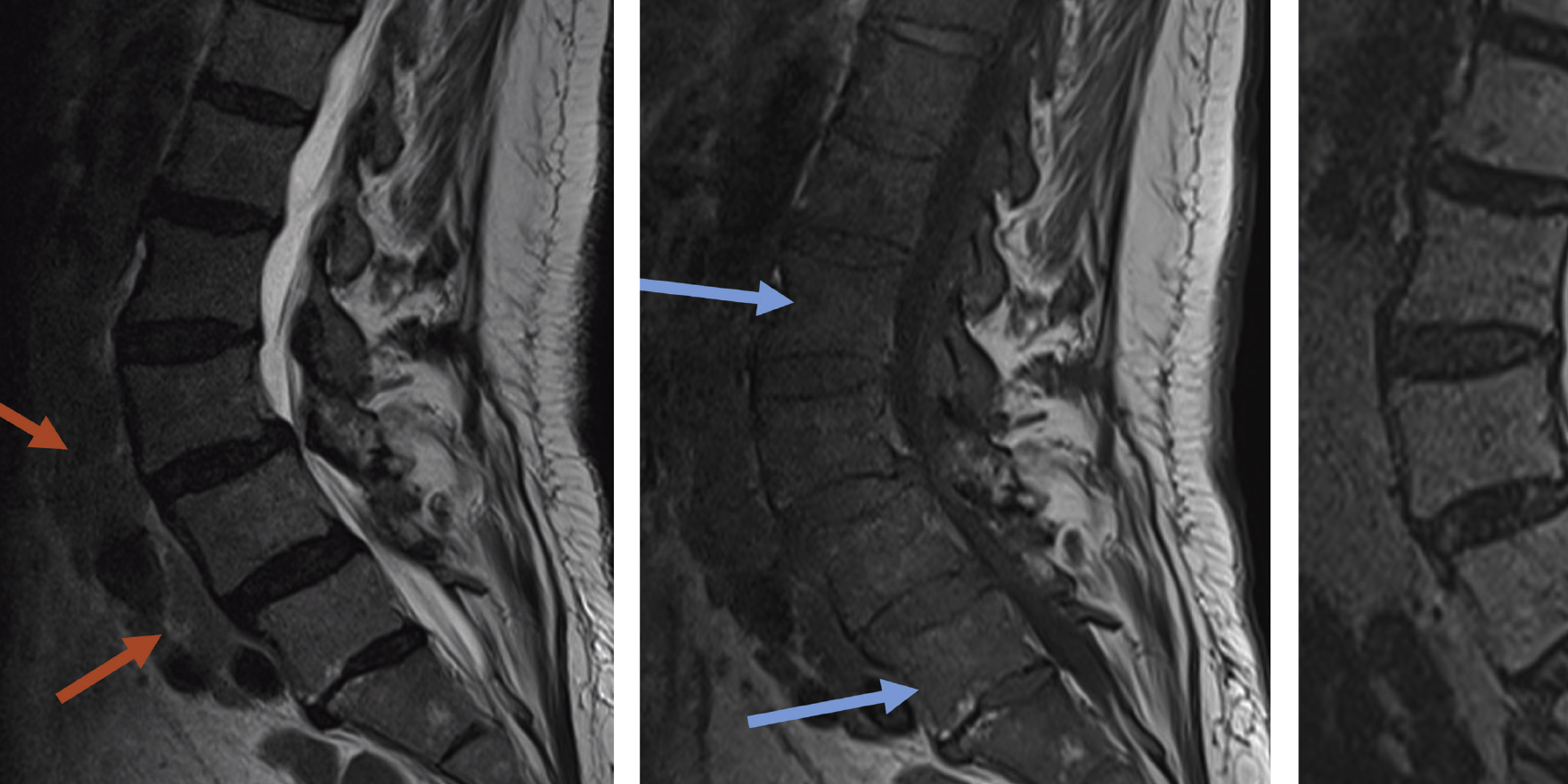
On the current MRI, there is evidence of interval surgery performed since 2011 at L3/4 on the right. At this level, increasing facet arthropathy and disc protrusion has resulted in severe canal stenosis and a worsening in the degree of left lateral recess stenosis. This is depicted on the axial and sagittal images.
Of particular note, there have been significant changes to the signal of the marrow throughout the lumbosacral axial skeleton. Specifically, the marrow appears lower in signal on T1 and T2 sequences, and hyperintense (bright) on STIR sequences. In addition, on closer inspection, there are multiple soft tissue nodular masses scattered along the retroperitoneum in a para-aortic location which were not present in 2011.
The low signal on T1 sequences, especially when this is darker/more hypointense than the intervertebral discs, would be highly concerning for marrow infiltration. Coupled with para-aortic lymphadenopathy, this would indicate either a haematological disorder, or alternatively a pelvic malignancy with metastatic disease.
DIAGNOSIS
The patient was eventually diagnosed with chronic lymphocytic leukemia (CLL). On review of the scout images (images used to plan the MRI), splenomegaly was also identified.
Vertebral marrow changes on MRI are common and often due to osteopenia or red marrow reactivation, however suspicion for pathological marrow infiltration is heightened when the marrow signal is equal or lower/darker than the adjacent disc on T1 imaging, and bright/hyperintense on STIR images.
This can be seen in the setting of metastases, myeloma, lymphoma, leukemias and for discitis/osteomyelitis.
Dr Sebastian Fung is a musculoskeletal radiologist who undertook an MRI imaging fellowship in Hospital for Special Surgery in New York. He now works in Sydney at St Vincent’s Private Hospital and Mater Hospital
Figure c – Sagittal STIR images from 2019 show corresponding high signal in the marrow
Figures d,e – Sagittal T1 (fig d) and T2 (fig e) showing tight canal stenosis at L3/4 due to disc protrusion and degenerative anterolisthesis on the prior 2011 MRI – but no lymphadenopathy. The marrow signal is that of normal yellow marrow (bright signal on T1 and T2)
Figure f: Axial T2 images of the 2019 MRI showing current canal stenosis and left lateral recess narrowing (blue arrow) . Note the numerous enlarged lymph nodes (red arrows)
figure g: showing previous 2011 MRI – no lymphadenopathy (red arrows)
Figure h: splenomegaly on scout image (red arrow)



